Clinical History
A routine blood test demonstrated isolated serum alkaline phosphatase (SAP) elevation in a 65yo male. There was no history of liver disease and other liver function tests were normal. Similarly, there was no history of Paget’s disease and apart from long standing knee arthritis, no further pain. There was mild warmth and bowing of the left tibia.
A bone scan was performed.
Scan Findings
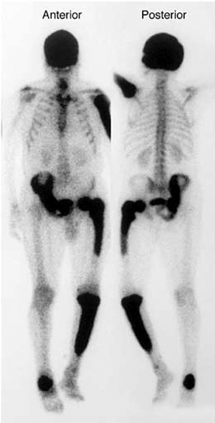
The bone scan (Figure One) demonstrates avidly increased uptake in the skull, left humerus, right hemipelvis, left femur, left tibia and right calcaneus. These findings are typical for active polyostotic Paget’s disease.
Discussion
Paget’s disease affects 1% of adults in developed countries. It is usually asymptomatic. Symptoms may include deep aching bone pain, deformity, fracture, arthritis (from articular involvement) and neurologic complications. Rarely, neoplastic transformation can occur. The cause of Paget’s disease is uncertain however the pathologic process is aggressive osteoclast-mediated bone resorption preceding imperfect osteoblast-mediated bone repair. An x-ray of a suspected area is often diagnostic and in many cases, the disease is often first identified on radiographs performed for an unrelated condition. Bone scans establish the distribution and extent of the disease, aid diagnosis and exclude other causes. Usually, the bone scan appearance is sufficient to differentiate other causes (such as skeletal metastatic disease – Figure Two) however this may be difficult in mono-ostotic disease. Late stage Paget’s disease may show minimal uptake on bone scans and in this situation, SAP may be normal; similarly SAP may be normal in mono-ostotic disease. Treatment with anti resorptive agents is recommended for: symptomatic cases; prophylaxis when affected sites suggest risk from progression – long bone fracture or nerve compression; elective surgery planned for a Pagetic site; or hypercalcaemia resulting from immobilisation. Serial SAP measurement usually suffices for follow-up.
Conclusion
Paget’s disease is one cause of SAP elevation. Bone scans are valuable in confirming Paget’s disease in suspected cases. Bone scans indicate disease distribution and extent and usually exclude other causes.
Case Study submitted by
Dr Scott Beuzeville
Department of Nuclear Medicine,
St. George Hospital.
(PDF DOWNLOAD)
Figure 1. Bone scan demonstrating typical features of Paget’s disease.
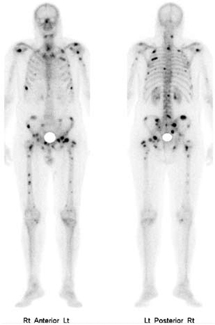
Figure 2. Bone scan demonstrating metastatic prostate cancer, which is an alternate cause for SAP elevation. Although the bone scan is abnormal, the pattern of abnormality is usually
sufficiently different from Paget’s disease to allow discrimination.